




In oral and maxillofacial surgery, incision and implant design can require suturing while placement of implant based on original anatomic position or operation properties. Last step of surgical operations that require incision/laceration is suturing.
Suture techniques are critical in surgery. At this point, it is vital to select appropriate material for traumatic surgical operations. When materials and methods to close the wound are inappropriate, normal healing process can become longer. Additionally, one of the few indicators that patients who completed oral surgery treatment to determine skills of the doctors is the look of sutured wound.
Generally, preference and habits of surgical doctor are effective in suture selection. Effective use of suture is only possible when the surgeon knows properties of needles and sutures and surgeons applies these in certain areas. (1)
Dental Suture
Suturing is an application to provide tissue integrity that decayed after surgical operation and controls resulting bleeding (2). Sutures are materials that are comprehensively and commonly used in all fields of surgery. (3)
Suture Materials
Needle Holder
This tool holds the needle while suturing. Handle part can be locked. These needle holders are available with thick and thin ends. Needle holder tip is shorter and stronger than hemostat. Part that holds the suture is staggered-tooth and enables stability. (4)
Needle
These are high-quality steel developed to pass the suture from tissue with minimal damage. Suture needles are available in wide range from small to large. Tips can be in round form like sewing needle or in triangle form. (Figure 1)
 Taper Point
Taper Point Square Body
Square Body Tapercutting
Tapercutting Reverse Cutting
Reverse Cutting CC Needle
CC Needle
Figure 1 – Needle Tip Types (4)
Needle shapes: These needles could be straight or curved. Curved type: These can be in 1/2, 1,4, 3/8, 5/8 or J shaped circle form. (Figure 2) (2, 4)
 1/4 Circle
1/4 Circle 3/8 Circle
3/8 Circle 1/2 Circle
1/2 Circle 5/8 Circle
5/8 Circle J-Shape
J-Shape
Figure 2 – Curved Needle Shapes (2)
Sutures
Selecting appropriate sutures may depend on biological structure of the wound and anatomic localisation. This selection is as important as technique and experience of the surgeon. Properties of ideal suture can be listed as follows:
- Perfect tension strength
- Easy to use
- Good know safety
- Minimum tissue reaction
- Compliance with tissue oedema or contraction
- Prevent infection
Things to Be Considered When Selecting Sutures
Tension Strength
This value is obtained by dividing weight that will cause suture to rip to cross-sectional area of the suture. This value is proportional with suture diameter. This value is standardised and numbered based on American Pharmacopeia. Numbering is as #/0. As number increases, diameter and tension strength decreases. (2) To enable wound closure in periodontal plastic surgery, minimum tension force should be applied on suture material.
Knot Strength
This is the force necessary to untangle the knot. This is related with slipperiness of the suture. (2)
Capillarity
This is related with physical configuration. Sutures have monofilament and multifilament structure. Twisted and braided structure of multifilament sutures enables ease-of-use however, micro cavities between filaments makes it easy for liquids to move along suture. This property is called capillarity. High capillarity means high infection risk. (2)
Elasticity
This is the property of the suture to get back to old form and length after tension. This way, suture stretches during tissue oedema and returns to old form after oedema disappears. (2)
Tissue Reaction
This is inflammation of wound tissue around suture. Since all suture materials are foreign, these sutures cause mild or severe reaction. Tissue reaction is peaked between day 2 and 7. This time and intensity of the reaction is related with suture type and amount. Multifilament cause higher tissue reaction than monofilaments and natural sutures cause higher tissue reaction than synthetic options. More than normal material within wound tissue will also increase infection risk. (2)
Suture Types for Absorption
Absorbable Sutures
These are operation sutures generally used to close dermis to decrease tension at the edges of epidermal wounds. High tension strength, absorption time, low tissue reaction, and good knot safety are important properties. There are synthetic and natural types: While natural sutures only have plain catgut and chromic catgut, synthetic absorbable ones include polyglycolic acid (PGA), polyglycolide lactic acid (PGLA), polydioxanone (PDO), and polyglycolide caprolactone (PGCL). (Table 1) (2, 5)
| Suture Type | Manufacturing Material | Tissue Support Time | Application |
|---|---|---|---|
| Plain catgut | Lamp small intestine mucosa. | 4 - 10 days | Used in fast healing mucosa. |
| Chromic catgut | Lamp small intestine mucosa processed with chromic acid. | 10 - 14 days | Used in fast healing mucosa. |
| Polyglycolic Acid (PGA) | Manufactured from polyglycolic acid, synthetic, multifilament | ~ 30 days | Used in subcutaneous sutures, mucosa, vein binding. |
| Polyglycolide Lactic Acid (PGLA) | Manufactured from 90% glycolide and 10% L-lactide, synthetic, multifilament | ~ 30 days | Soft tissue closure and binding. |
| Polydioxanone (PDO) | Manufactured from polyester, synthetic, monofilament | ~ 60 days | Used in paediatric cardiovascular tissues and ophthalmic structures. |
| Polyglycolide Caprolactone (PGCL) | Manufactured from 75% glycolide and 25% co-caprolactone, synthetic, monofilament | ~ 7 days | Used in closure of surface wounds |
Table 1 – Absorbable Sutures (5)
Non-Absorbable Sutures
These sutures are durable against proteolysis and hydrolysis. These sutures can have tension strength on 60th day. Non-absorbable suture types: silk, nylon polyamide (PA), polypropylene (PP), polyester polytetrafluoroethylene (PTFE), and stainless steel. (Table 2)
| Suture Types | Manufacturing Material | Tissue Reaction: | Application |
|---|---|---|---|
| Silk | Knitted, silkworm cocoon | High | Used for soft tissue closure and vein binding. |
| Nylon Polyamide (PA) | Nylon 6 or Nylon 6.6 monofilament, long-chain aliphatic polymer | Low | Used for skin closure, soft tissue closure and binding. |
| Polypropylene (PP) | This is a synthetic linear polyolefin formed from stereoisomer of isotactic crystal of polypropylene. | Low | Used for very flexible skin closure and vein anastomosis. |
| Polyester (PTFE) | This suture is obtained from long-chained, linear polyester with high molecular weight. | Low | These sutures are used in general soft tissue coating and bonding of cardiovascular, ophthalmic, or neuro surgical applications. |
Table 2 – Non-absorbable Sutures (5)
Silk is commonly preferred by surgeons. These sutures are manufactured from natural proteins obtained from silkworm cocoon. Silk is multifilament (naturally braided) and these sutures are perfect for usage, suturing, and knotting. Since it is natural fibre, this suture doesn’t cause significant tissue inflammation. It has high capillarity. Elasticity and plasticity are low. To understand the product easily, there are necessary information on suture packages for surgeons. (Figure 3) (2, 5)

Figure 3 – Suture fabrication tag information (2)
Suture Principles
Needle holder should hold the needle at 1/3 back of the needle. Needle should be applied with a right angle (90º). This way, tissue ruptures are prevented. Tissue should pass from the tissue with its own curve to prevent rupture. Needle should be pricked at least 3 mm away from both sides of wound tissue and to same dept. If two sides of the wound has different thickness, needle should be pricked from thin side to thick side. While suturing, tissue should not be pulled and stretched. If tissues are sutures by stretching, stiches will open. If know is too tight, tissue may rupture and cause ischemia. Knots should be on incision line. Each knot should have 3-4 mm between them.
While suturing, corners or papilla are sutured first, and vertical and horizontal incisions are sutured later. If one of the wound sides is upright, knot is positioned on the stable side, tightened, and both sides of the wound are levelled. If tissues have different thickness, suturing should be deeper on the thinner side or needle should be pricked from further of incision in thin side, and two sides of the wound should be connected.
If there is no special case, sutures are removed in 5-7 days. When sutures are removed, suture is hold and pulled upwards with a dental tweezer or forceps and one side of the suture beneath knots are cut. Before removing sutures, it is recommended to rinse the mouth with anti-septic. (4) To decrease tension between flap edges, before suturing, flap tissue should be positioned into designed area in passive form. Tissue trauma such as tension, rupture, or distortion should always be avoided. Gentle and careful manipulations with micro surgical instruments are beneficial.
Since each suture causes extra damage around wound edges, possibly lowest number of sutures should be applied. 6/0 and 8/0 non-resorbed suture material should be selected. Resorbable material be selected for multi-layered closure. Sutures should not act as ligatures and minimum tension should be applied. (6)
Dental Suture Suturing Types
Simple Suture
This is the most common suture technique within mouth cavity. Suture passes from one side of the wound, exits from the other side, and knotted at the top. (Figure 4) (4)

Figure 4 – Simple Suture Technique (4)
Vertical Mattress Suture
Vertical mattress suture technique is applied in two stages especially on tissue on skin. (Figure 5) (4)

Figure 5 – Vertical Mattress Suture Technique (4)
Horizontal Mattress Suture
Horizontal mattress suture technique tightens both sides of the wound. This is beneficial to close soft tissues. This is the easiest way to fix two papilla with single knot. (Figure 6) (4)

Figure 6 – Horizontal Mattress Suture Technique (4)
8 Figure Suture
This is a modified version of horizontal mattress suture. While closing both side of the soft tissue, 8 sutures helps preserving the position of clot. (Figure 7) (4)

Figure 7 – 8 Suture Technique (4)
Continuous Suture
If there is long incision, continuous suture technique is preferred. In this technique, instead of applying a knot every time, long incision line can be sutured in a short time. This could have knotted style or simple technique. (Figure 8) Disadvantage of continuous suture is when there is a rupture, suture below can loosen. (4)

Figure 8 – Continuous Suture Technique (4)
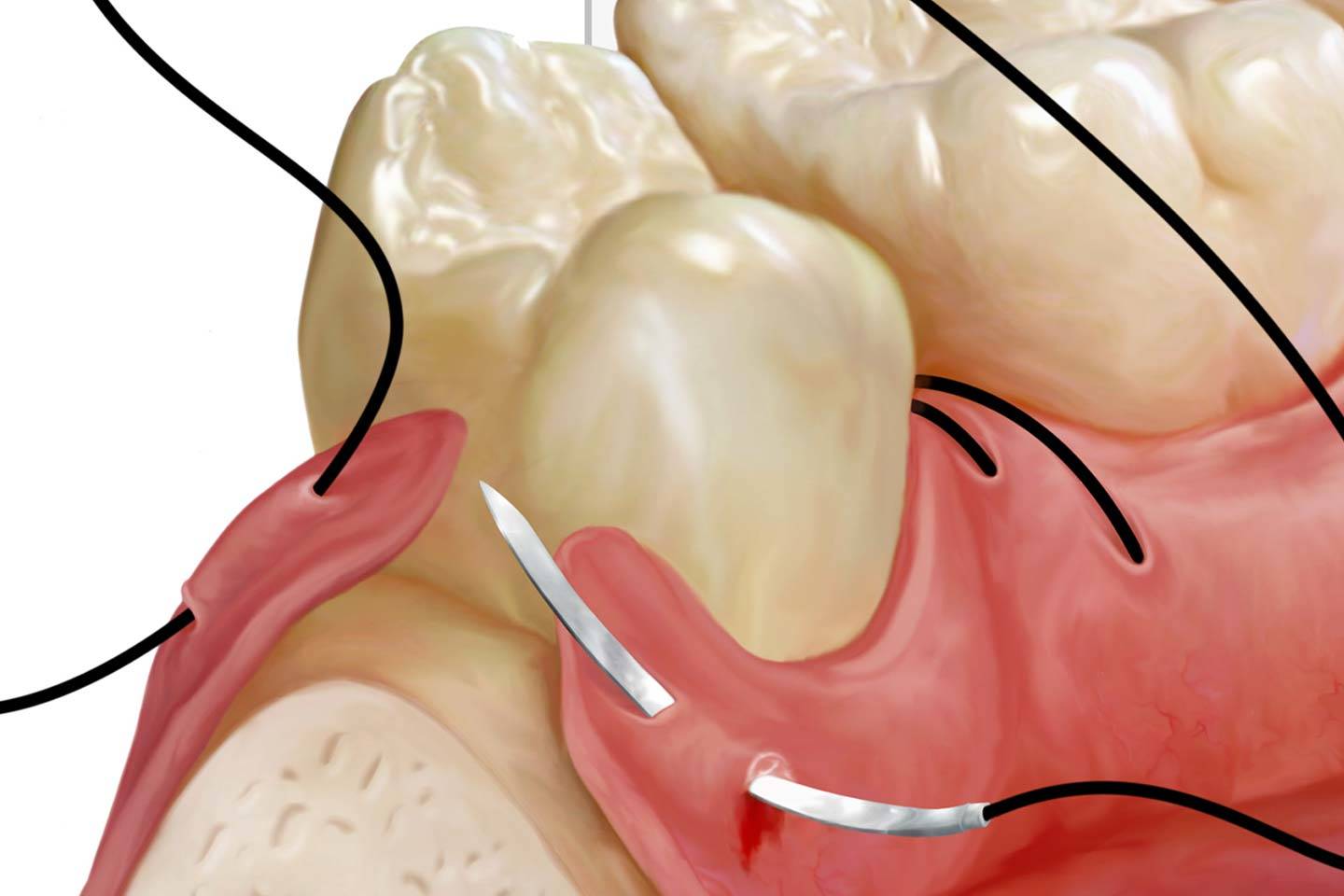
Sling Suture
When surgical operations are applied on limited regions, for example, if lambo is lifted from one side, this suture technique is common. This is also applied when buccal and lingual flaps are desired to be placed on different positions. Needle passed from hemisects of tooth to outer surface of buccal flap, perambulates the teeth and passed from palatial flap in distal. Suture is brought back to hemisects where suture starts, passed from internal surface of buccal flap, and knotted. (Figure 9) (7)

Figure 9 – Sling Suture Technique (8)
First step of most surgical operations is incision. A surgeon holding the bistoury should know what to do, localisation of anatomic structures around operation field, and creating maximum effect with minimum trauma after the intervention. Following the incision, infection around operation field should be post-operatively prevented and suturation should be applied to close the wound to provide high-comfort to patient. Closure of wound is as important as incision. Therefore, in addition to experience and skills of the surgeon, material knowledge is required. In this article, information regarding common suture operation techniques and used materials which will be used are presented and explained for dentist.
To view articles, posts, and technical details regarding suture use in other surgical operation, you can use our website. Additionally, you can select and view dental suture products of Boz Medical. You can click here for your orders and support. Our sales representatives will be happy to answer all your questions and meet your demands.
Bibliography
(1) Alpaslan G. H. İNSİZYON SÜTÜR VE FLEP TEKNİKLERİ, Gazi Üniversitesi Diş Hekimliği Fakültesi • Ağız Diş ve Çene Hastalıkları Ana Bilim Dalı, 4. Sınıf Ders Notları, ANKARA
(2) Altınyazar H. C., Koca R. DERMATOLOJİK CERRAHİDE SIK KULLANILAN SÜTÜR MATERYALLERİ, Zonguldak Karaelmas Üniversitesi Tıp Fakültesi • Dermatoloji Anabilim Dalı, ZONGULDAK, 2004.
(3) Parirokh M, Asgary S, Eghbal M J, Stowe S , Kakoei S. A SCANNING ELECTRON MICROSCOPE STUDY OF PLAQUE ACCUMULATION ON SILK AND PVDF SUTURE MATERIALS IN ORAL MUCOSA, International Endodontic Journal, 2004; 37:776–781
(4) Türker M, Yücetaş Ş. AĞIZ DİŞ ÇENE HASTALIKLARI VE CERRAHİSİ, Üçüncü baskı, ANKARA, 2004.
(5) Akça T., Mersin Üniversitesi Tıp Fakültesi • Genel Cerrahi Anabilim Dalı, 4. Sınıf Ders notları, MERSİN.
(6) Velvart P, Peters C, Peters O A. SOFT TISSUE MANAGEMENT: SUTURING AND WOUND CLOSURE, Endodontic Topics 2005; 11:179–195
(7) Evrenesoğlu E., Ege Üniversitesi Diş Hekimliği Fakültesi • Periodontoloji Ana Bilim Dalı, 4. Sınıf Ders Notları, İZMİR.
(8) Jansson L, Sandstedt P, Laftman AC, Skoglund A. RELATIONSHIP BETWEEN APICAL AND MARGINAL HEALING IN PERIRADICULAR SURGERY Oral Surgery, Oral
Medicine, Oral Pathology, Oral Radiology, and Endodontology, 1997; 83 :596–601



